

Presenter: Peter Vitulli Jr. D.O. Third year resident, Chris Manlio D. O. first year resident
Dermatology Program: North Broward Hospital District
Program Director: Stanley E. Skopit D.O.
Submitted on: Nov 30, 2003
CHIEF COMPLAINT: Fever, malaise, and a skin rash with suspected bacteremia
CLINICAL HISTORY: A 17-year-old Hispanic female was admitted to the hospital with fever, malaise, and a widespread skin rash suggestive of bacteremia. Initially, she experienced pruritus followed by burning pain in her skin, which worsened with movement. She reported a fever reaching 103.7°F, along with nausea, anorexia, and malaise.
The patient had a history of psoriasis, previously controlled with mid- to high-potency topical steroids and Dovonex ointment. Approximately six days prior to admission, she was seen by her dermatologist for worsening psoriasis, presenting with multiple erythematous macules in the flexor areas and silvery plaques on the extensor surfaces of her elbows and knees. She was started on triamcinolone 0.1% cream and Dovonex ointment, both to be applied twice daily. Over the next six days, her rash spread extensively, leading to the formation of pustules and prompting her pediatrician to admit her to the hospital.
PHYSICAL EXAM:
Temp 103.1, Heart rate 104, Respiratory rate 18, Blood pressure 108/62
Gen: Awake, Alert, Oriented X 4, ill-appearing female with guarding of movement secondary to pain.
Skin: Diffusely erythrodermic with multiple pustules confluent to lakes of pus on the trunk, face, and extremities. Multiple areas of denuding skin were noted. A mild fecal odor was noted.
HEENT: Neck was supple, oral phary7nx was noted to have slight erythema and mild fissuring of the lips.
The remainder of exam was unremarkable.


LABORATORY TESTS:
Abnormalities on Day 1 WBC 18.4, Hb 11.2, Hct 33.4.
Day 7 WBC 10.9 Hb 11.8 Hct 34.2 remainder of blood work including liver functions were normal.
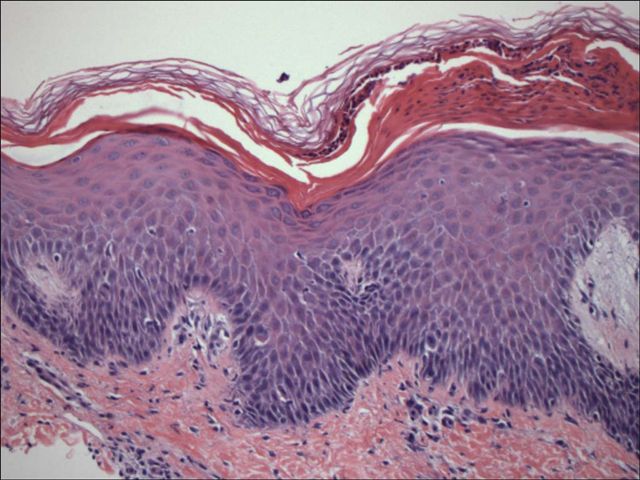
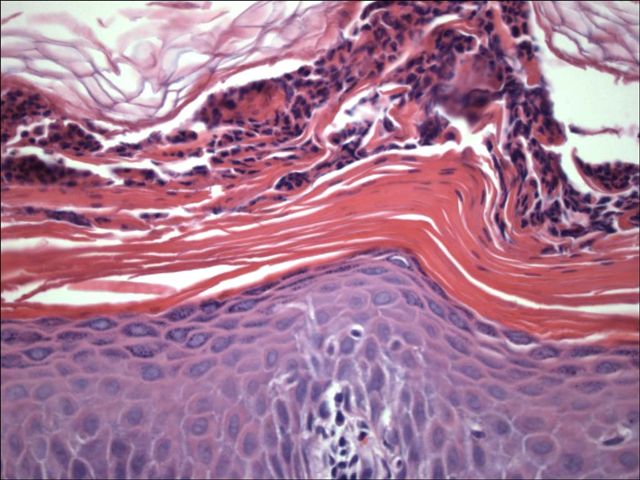
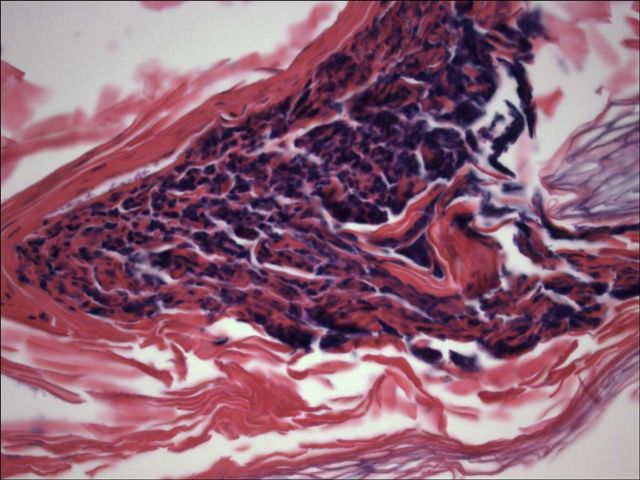
DERMATOHISTOPATHOLOGY:
Skin biopsy revealed parakeratosis, prominent Munro’s microabscesses, focal spongiform pustule formation, and superficial and deep polymorphous infiltrate, containing multiple polymorphonuclear leukocytes, psoriasiform acanthosis, and papillary dermal telangiectasia and edema.
DIFFERENTIAL DIAGNOSIS:
1. Pustular Psoriasis
2. Steven’s Johnson’s Syndrome
3. TEN
4. Kawasaki’s Disease
5. Acne Fulminant


