

Presenter: Jocelyn E. Harris, DO
Dermatology Program: Lehigh Valley Hospital
Program Director: Stephen Purcell, D.O.
Submitted on: Dec 11, 2003
CHIEF COMPLAINT: A progressively enlarging papule on the patient’s left cheek
CLINICAL HISTORY: Patient presented to clinic for a lesion with no discharge and was neither tender nor pruritic. She denied any history of similar lesions. She also denied fever, night sweats, heat/cold intolerance, and weight fluctuation. Upon initial presentation to her primary care physician, a diagnosis of an irritated epidermal cyst was made and she was prescribed three courses of azithromycin. Incision and drainage by her PCP failed to express any culturable material or cause the lesion to involute.
PHYSICAL EXAM:
Clinical examination revealed a 1.2 cm erythematous, slightly movable, firm nodule with a central crust located in the left malar area, directly below the infraorbital prominence. No pre- or post-auricular, cervical or supraclavicular lymphadenopathy was appreciated. Evaluation of the head, neck, nares, and oral mucosa revealed no other suspicious lesions.

LABORATORY TESTS:
A 3 mm punch biopsy was taken from lesion. The biopsy findings prompted a complete radiological workup, including MRI and CT scans of the head and neck. MRI studies of the head demonstrated a 1.7 x 2.0 cm nodule in the left malar region, with subcutaneous and underlying skeletal muscle invasion. No hypervascularity or bone involvement was observed. A second focus of a similar signal, measuring 2.4×1.2×1.7 cm, was seen inferior and slightly medial to the right submandibular gland. Additionally, there was significant lymphadenopathy detected bilaterally in the submandibular chains. CT evaluation also confirmed the secondary focus noted in the right submandibular region, at the level of the hyoid. Chest x-rays were unremarkable.
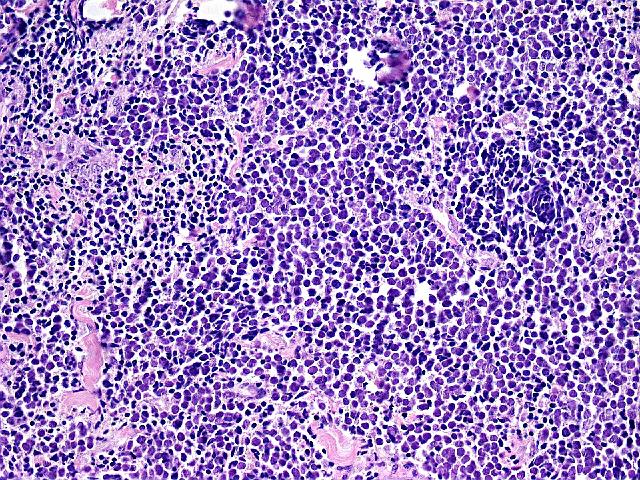
DERMATOHISTOPATHOLOGY:
Histologic examination of the punch biopsy revealed variously sized and shaped aggregates of neoplastic cells with finely granular nuclei and scant cytoplasm. The cells displayed an infiltrating growth pattern throughout the dermis, subcutis, and skeletal muscle. Furthermore, many mitoses and necrotic cells were noted. Immunohistochemical stains were positive for CK20, CD45, chromogranin A, and focally positive for low-molecular-weight keratin subtypes. Stains for S-100 antigen were negative.
Right sentinel lymph node biopsy showed elaborate branching papillae with ovoid, hyperchromatic nuclei, nuclear grooves, and intranuclear inclusions. Numerous psammoma bodies were also present. The biopsy showed thyroglobulin immunoperoxidase positivity.
DIFFERENTIAL DIAGNOSIS:
1. Squamous cell carcinoma with nodal metastasis
2. Squamous cell carcinoma with metastatic papillary thyroid carcinoma
3. Merkel cell carcinoma with nodal metastasis
4. Merkel cell carcinoma with metastatic papillary thyroid carcinoma


