
Presenter: Jennifer Bucci, DO & Schield Wikas, DO, FACOD
Dermatology Program: Cuyahoga Falls General Hospital
Program Director: Schield Wikas, DO
Submitted on: July 4, 2006
CHIEF COMPLAINT: Rash on bilateral upper extremities and face for several months
CLINICAL HISTORY: This is a case of a 39-year-old Caucasian female who presented with a skin rash of several months duration on the bilateral upper extremities and face. She later developed many extracutaneous manifestations including xerostomia, dysphagia, fatigue, anorexia with subsequent weight loss, and paresthesias of the bilateral lower extremities. Most disconcerting to her, however, was an accelerating loss of motor function; she had difficulty getting out of a chair and walking upstairs. She has tried topical steroids for the rash without signs of improvement.
Over the next several months the patient developed a generalized induration of the skin over the anterior and posterior shoulders. The patient exhibited sclerodactyly with the decreased movement of the bilateral metacarpal phalangeal, proximal, and distal interphalangeal joints. Microstomia, however, was not appreciable on physical examination. The left parietal scalp had diffuse hair thinning without evidence of cicatricial alopecia. The hairs did not have increased fragility. She had progressive weight loss recorded on evaluations prior to the onset of therapy.
Other information: Barium esophagogram revealed incomplete relaxation of the cricopharyngeus muscle. Electromyography revealed acute generalized myositis that was moderate to severe in nature involving both proximal and distal musculature. Computerized tomography (CT) scan of the abdomen and pelvis showed no acute pathology. Bone marrow aspiration and biopsy were essentially non-diagnostic. Plasma cells accounted for less than five percent of marrow cellularity. The thyroid scan revealed a mild elevation in uptake. Thyroid ultrasound revealed a non-enlarged gland with multiple tiny colloid cysts and foci of calcification.
PHYSICAL EXAM:
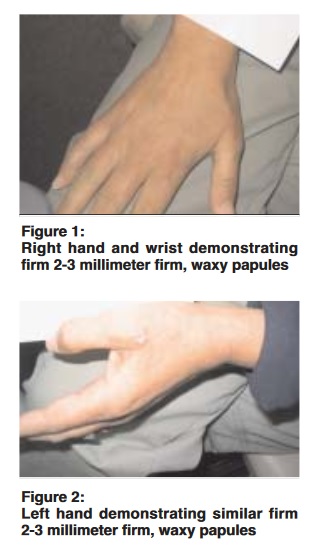
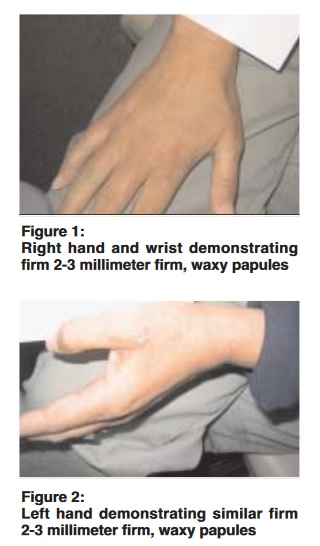
On physical examination patient was a Caucasian female approximately 67 inches tall and weighed 160 pounds. The bilateral dorsal hands and wrists had 2-3 millimeter firm, waxy papules present symmetrically in no particular arrangement. (See figures 1 and 2). The range of motion in the joints of the hands or wrists was not limited and there was no associated induration. The similar firm, waxy papules were present on the preauricular face and along the nasal sidewall symmetrically. There was a mottled pigmentary change of the skin, noted especially over the bilateral lower extremities, consistent with livedo reticularis. Pulses were easily palpable over distal arteries in the lower extremities. Neurologic examination was unremarkable except slightly diminished reflexes at the ankle.
LABORATORY TESTS:
Antibody screening was negative for antinuclear antibody (ANA), anti-double-stranded DNA (anti ds-DNA), rheumatoid factor (RF), SSA and SSB antibodies, and scl-70. Serum protein electrophoresis (SPEP) confirmed an IgG kappa monoclonal gammopathy. Quantitative immunoglobulins were within normal limits. Thyroid studies revealed hypothyroidism. Thyroid-stimulating hormone (TSH) was elevated at 10.956 and triiodothyronine (T3) was decreased at 248. Muscle enzymes were elevated included creatinine phosphokinase (CPK) at 585, lactate dehydrogenase (LDH) at 230, and aldolase at 17.2, as well as an erythrocyte sedimentation rate (ESR) at 57.
DERMATOHISTOPATHOLOGY:
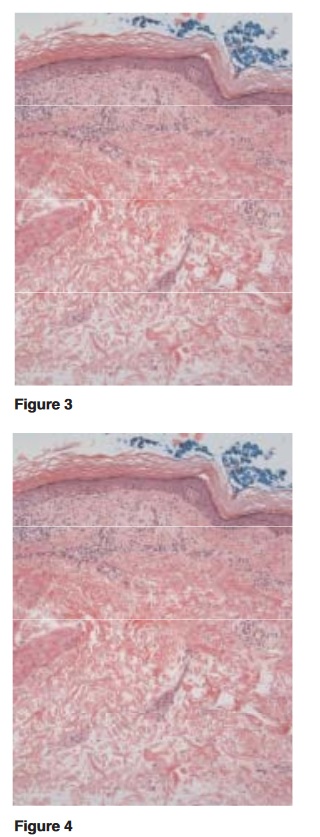
A skin biopsy taken from the right hand prior to the onset of therapy was a punch specimen. The changes were compatible with lichen myxedematosus. The epidermis was intact with a dermal proliferation of fibroblasts and increased interstitial mucin confirmed with a colloidal iron stain.
DIFFERENTIAL DIAGNOSIS:
1. Papular mucinosis
2. Nephrogenic fibrosing dermopathy
3. Scleredema
4. Generalized myxedema


