
CORRECT DIAGNOSIS:
Idiopathic Recurrent Palmoplantar Hidradenitis
DISCUSSION:
Idiopathic Recurrent Palmoplantar Hidradenitis (IRPH), first described in 1988 by Metzker and Brodsky, has also been described as Idiopathic Palmoplantar Hidradenitis, Palmoplantar Hidradenitis, and Palmoplantar Eccrine Hidradenitis. It begins abruptly with a few, small tender plantar and occasionally palmer erythematous nodules. These progress in size (up to 3 cm) and number (up to 15) to and become increasingly painful, often becoming disabling. Approximately 50 cases have been described in the literature; however, there is a great deal of discrepancy over both the clinical and histological characteristics of the dermatoses that have been included under the rubric of IRPH.
IRPH most commonly presents in children and young adults and is self-limited. Authors have proposed a myriad of precipitating factors including hyperhidrosis, trauma, physical activity, exposure to wet footwear, and oropharyngeal streptococcal infection. One author suggested a bi-modal seasonal predilection for the spring and autumn. Most patients are without other symptoms although low-grade fever has been reported. The underlying pathology is poorly understood.
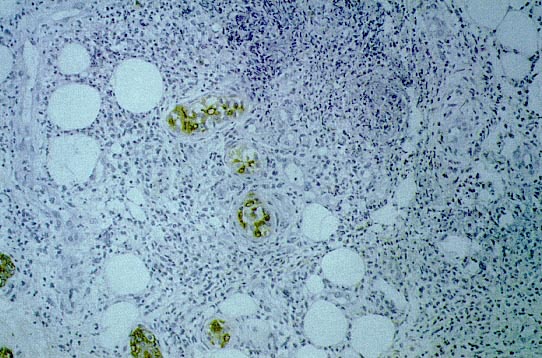
The primary histopathologic finding in IRPH consists of a nodular neutrophilic infiltrate localized to the eccrine coils with a slight extension to the periglandular tissue. The infiltrate occasionally forms well-circumscribed focal abscesses. In the mid to deep dermis, there may be a mild perivascular infiltrate of neutrophils, lymphocytes, and few histiocytes. Extravasated erythrocytes may be present. There has been no evidence of leukocytoclastic vasculitis, eccrine syringosquamous metaplasia, or microorganisms; including bacteria and fungi. The straight dermal eccrine ducts, acrosyringia, and epidermis are typically spared.
The clinical differential diagnosis includes Sweet’s syndrome, traumatic plantar urticaria, atypical erythema nodosum, atypical erythema multiforme, Behcet’s disease, and chilblains.
TREATMENT:
IRPH runs a benign self-limited course although recurrences have been reported. Many treatments have been reported, including systemic antibiotics, systemic steroids, nonsteroidal anti-inflammatory drugs (NSAIDs), and potassium iodide solution. Most authors agree that bed rest and symptomatic treatment with NSAIDs is adequate as the lesions typically resolve over approximately one to two weeks.
We treated our patient expectantly with bed rest and NSAIDS and her lesions began to resolve in five days and completely resolved over the following week. She has not had a recurrence.
REFERENCES:
1. Rabinowitz LG, et al. Recurrent Palmoplantar Hidradenitis in Children. Arch of Derm 1995; 131(7): 817-20
2. Simon M, et al. Idiopathic Recurrent Palmoplantar Hidradenitis in Children: Report of 22 Cases. Arch of Derm1998;134(1):76-79
3. Landau M, et al. Palmoplantar Eccrine Hidradenitis: Three New Cases and Review. Ped Derm 1998;15(2):97-102
4. Naimer SA et al. Plantar hidradenitis in children induced by exposure to wet footwear. Ped Emerg Care 2000;16(3):182-183


