

Presenter: Vienna Lowenbraun, D.O.
Dermatology Program: Genesys
Program Director: Kimball Silverton, D.O.
Submitted on: April 30, 2013
CHIEF COMPLAINT: Diffusely “dry and itchy” skin.
CLINICAL HISTORY: A 74-year-old Caucasian male presented with complaint of four and a half months of diffusely “dry and itchy” skin. He noted that the skin changes began suddenly; first noticing the dryness on his arms, and within several days notice that it had become diffuse. He stated that he first noticed the changes two weeks after using a degreasing agent to clean his refrigerator coils and was concerned that the solvent was the source of his xerotic and pruritic skin. Several weeks prior to presenting to our clinic, he sought care at his primary care physician’s office for the same complaints. His primary care physician diagnosed him with having xerosis and was advised to apply Aquaphor twice daily.
Other information: The patient’s medical history included type II diabetes mellitus, hypertension, hypercholesterolemia, and coronary artery disease. Recent routine colonoscopy revealed polyps without signs of malignancy. A review of systems was positive for sixteen-pound weight loss in the last two months, a recent change in taste (constantly bitter), and intermittent diarrhea for one month. His medications included furosemide, carvedilol, lisinopril, ezetimibe and simvastatin, aspirin, loratadine, insulin glargine, and insulin lispro. No new medications were started for several months prior to the patient developing his cutaneous symptoms.
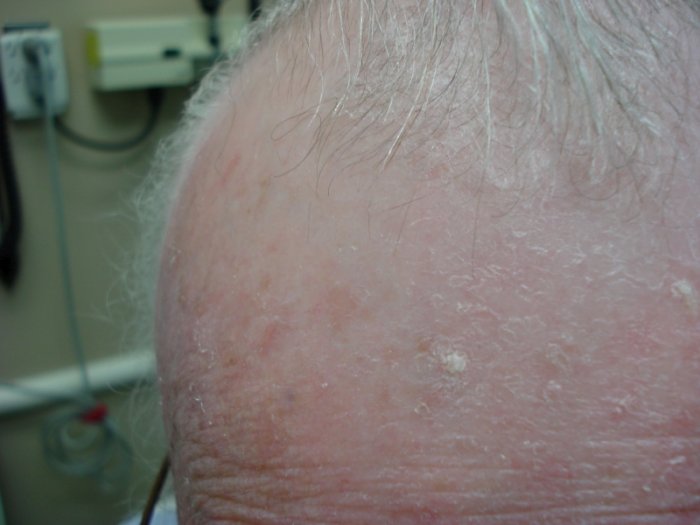
PHYSICAL EXAM:
On physical exam, the patient’s integument was diffusely rough, xerotic, and superficially scaly with sparing of the axilla, groin, soles, and infra-mammary region. There was the prominence of skin creases over the palms as well as a mosaic patterned superficial scale present on bilateral upper thighs. The scalp was non-scaly, smooth, and shiny with a cigarette-paper-like appearance upon manipulation.








LABORATORY TESTS:
Baseline CBC and CMP were ordered with the following abnormalities: Absolute eosinophils 9032, cell morphology positive for rouleaux cells and anisocytes.
DERMATOHISTOPATHOLOGY:
The results of the punch biopsy from the left forearm revealed a sparse superficial perivascular infiltrate of lymphocytes present around slightly ectatic vessels. The cornified layer was composed of variably compact orthokeratosis. There was no evidence of fungal hyphae on PAS stain.
DIFFERENTIAL DIAGNOSIS:
1. Aquired Icthyosis
2. Paraneoplastic dermatitis
3. Xerosis
4. Eczema craquele
5. Seborrheic Dermatitis


