CORRECT DIAGNOSIS:
Telangiectasia macularis eruptiva perstans
DISCUSSION:
Telangiectasia Macularis Eruptiva Perstans (TMEP) is part of the mastocytosis disease spectrum, which is characterized by the abnormal accumulation of normal mast cells. This cutaneous disease was first described by Parkes Weber in 1930. Today there are three major forms of cutaneous mastocytosis recognized by the World Health Organization. These include: urticaria pigmentosa, diffuse cutaneous mastocytosis and mastocytoma. TMEP is considered a rare subvariant of urticaria pigmentosa, found in less than one percent of patients with mastocytosis. TMEP typically presents in adults, however, cases involving children have been reported. Mastocytosis involves the skin in approximately 80% of cases, therefore patients commonly present with a cutaneous disease but can present with systemic disease.3 Other organs commonly effected include: bone marrow, liver, and gastrointestinal tract.
Mastocytosis occurs when there is an accumulation of mast cells in various organs. Multiple studies have proposed that mast cell hyperplasia occurs when a c-kit proto-oncogene mutation is observed. This mutation plays a roll in mast cell survival and proliferation. Mast cells have an important role in the bodies inflammatory process, storing and releasing the chemical mediators histamine, tryptase, TNF-α, leukotrienes, prostaglandins, platelet-activating factor, heparin, and IL-8. Patients with mastocytosis can experience urticaria, blistering, wheezing, diarrhea, flushing, and hypotension when mast cells release large quantities of histamine and other chemical mediators.
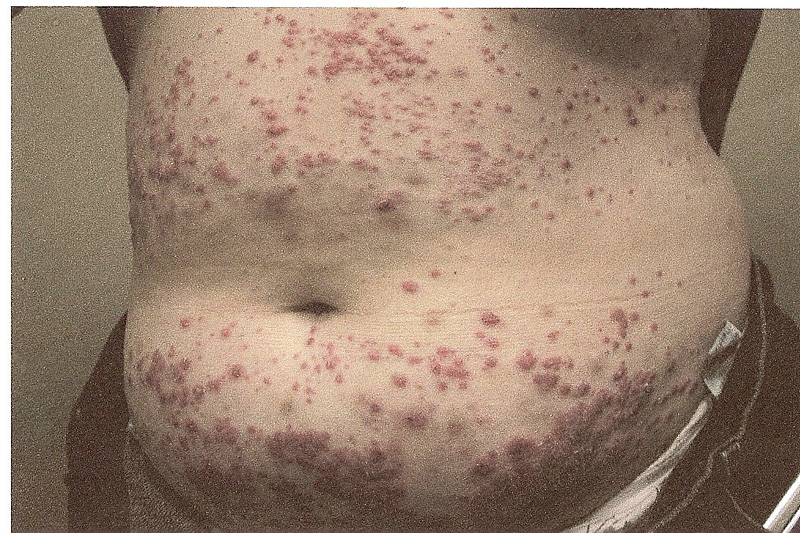
Clinically TMEP presents as reddish-brown macules with telangiectasis. These lesions regularly involve the trunk but can be found on the face and extremities.8 Lesions of TMEP most commonly do not display Darier’s sign. Using dermoscopy lesions of TMEP exhibit linear vessels in a reticular pattern. The diagnosis of TMEP is often confirmed by analyzing skin biopsies using special stains. The histopathological features of TMEP demonstrate an infiltrate of spindle-shaped mast cells, primarily located in the upper third of the dermis, clustered around dilated capillaries and venules. It is crucial to stain sections of suspected mastocytosis with Giemsa or Toludine-blue stains as the infiltrates can be difficult to identify with a Hematoxylin and Eosin stain. It is also important to measure serum tryptase levels in patients suspected of having mastocytosis. Tryptase is a chemical mediator secreted from mast cells, therefore it is believed that an elevated level can help determine if a patient has a systemic mastocytosis. Patients that have cutaneous mastocytosis without systemic involvement often have normal or slightly elevated tryptase level, while an increase in tryptase level may indicate multi-organ involvement. Adults with an elevated tryptase level should undergo further testing including a bone marrow examination.
TREATMENT:
To date, there is no gold standard treatment for TMEP or cutaneous mastocytosis. Initial management is to instruct patients to avoid extreme temperatures, shellfish, alcohol, and aspirin which are known to stimulate mast cell degranulation.5 The initial medical treatment for discomfort includes antihistamines, specifically H1 and H2 receptor antagonists. These medications can help control flushing, urticaria and gastric acidity.7
In severe cases, glucocorticoids are recommended.2 Improvement of symptoms and regression of skin lesions has also been seen with the use of psoralen plus ultraviolet light.2 Several treatments have been used with mixed results including Ketotifen, doxepin, cromolyn sodium, leukotriene antagonists, alpha interferon.9, 11
REFERENCES:
Parkes Weber, F., & Hellenschmied, R. (1930). Telangiectasia macularis eruptiva perstans. British Journal of Dermatology and Syphilis, 42, 374–382.
Valent, P., Akin, C., Sperr, W. R., et al. (2005). Mastocytosis: Pathology, genetics, and current options for therapy. Leukemia & Lymphoma, 46(1), 35–48. https://doi.org/10.1080/10428190410001687403
Akin, C., & Metcalfe, D. D. (2004). Systemic mastocytosis. Annual Review of Medicine, 55, 419-432. https://doi.org/10.1146/annurev.med.55.102403.093953
Sotiriou, E., Apalla, Z., & Ioannides, D. (2010). Telangiectasia macularis eruptiva perstans successfully treated with PUVA therapy. Photodermatology, Photoimmunology & Photomedicine, 26(1), 46-47. https://doi.org/10.1111/j.1600-0781.2009.00459.x
Tebbe, B., Stavropoulos, P. G., Krasagakis, K., & Orfanos, C. E. (1998). Cutaneous mastocytosis in adults. Dermatology, 197(2), 101–108. https://doi.org/10.1159/000017263
Yarden, Y., Kuang, W. J., Yang-Feng, T., Coussens, L., Munemitsu, S., Dull, T. J., Chen, E., Schlessinger, J., Francke, U., & Ullrich, A. (1987). Human proto-oncogene c-kit: A new cell surface receptor tyrosine kinase for an unidentified ligand. EMBO Journal, 6(11), 3341-3351. https://doi.org/10.1002/j.1460-2075.1987.tb02588.x
Kutlubay, Z., Yardımcı, G., Engin, B., & Tuzun, Y. (2011). Cutaneous mastocytosis. Journal of Turkish Academy of Dermatology, 5(3), 1-6. https://doi.org/10.6003/jtad.1451a2
Gibbs, N. F., Friedlander, S. F., & Harpster, E. F. (2000). Telangiectasia macularis eruptiva perstans. Pediatric Dermatology, 17(3), 194-197. https://doi.org/10.1046/j.1525-1470.2000.00194.x
Costa, D., Moura, H., Rodrigues, R., Pineiro-Maceira, J., & Ramos-e-Silva, M. (2011). Telangiectasia macularis eruptiva perstans, a rare form of adult mastocytosis. Journal of Clinical and Aesthetic Dermatology, 4(10), 52–54. PMID: 22059194
Akay, B. N., Kittler, H., Sanli, H., Harmankaya, K., & Anadolu, R. (2009). Dermatoscopic findings of cutaneous mastocytosis. Dermatology, 218(3), 226–230. https://doi.org/10.1159/000193779
Cengizlier, R., et al. (2009). Treatment of telangiectasia macularis eruptiva perstans with montelukast. Allergology and Immunopathology, 37(5), 245-247. https://doi.org/10.1016/j.aller.2009.05.002