

Presenter: Christian W. Oram, D.O.
Dermatology Program: Lehigh Valley Health Network/Philadelphia College of Osteopathic Medicine
Program Director: Stephen M. Purcell, D.O.
Submitted on: June 2, 2013
CHIEF COMPLAINT: Lesion on the right breast
CLINICAL HISTORY: The patient presented in October 2010 with a pink to purple asymptomatic plaque on the right medial breast. The lesion had developed in an area of previous radiation treatment for breast cancer. Since the lesion arose in an area of previous radiation treatment, a biopsy was obtained. The lesion remained asymptomatic and stable in size for approximately one year. No treatment was pursued and watchful waiting was implemented, with the intent to biopsy any new or changing areas. At approximately twelve months, within the span of two weeks, the lesion grew four times in size and became tender. This prompted re-biopsy due to the aggressive clinical nature of the lesion.
PHYSICAL EXAM:
October 2010: 2.0 x 3.0 cm pink to purple plaque on the right breast.

December 2011: 10.0 x 14.0 cm pink to purple, indurated plaque on the right breast.

LABORATORY TESTS: N/A
DERMATOHISTOPATHOLOGY:
Advanced Dermatology Associates, LTD. (AD10-10799, 10/04/2010) Right medial breast: “In the superficial half of an edematous dermis is a subtle population of ectatic vessels with plump, but small, endothelial cells. This is somewhat obscured by a patchy mixed cell inflammatory infiltrate that includes lymphocytes, histiocytes, and a rare eosinophil. There are also extravasated erythrocytes. A PAS stain is negative for fungus.”
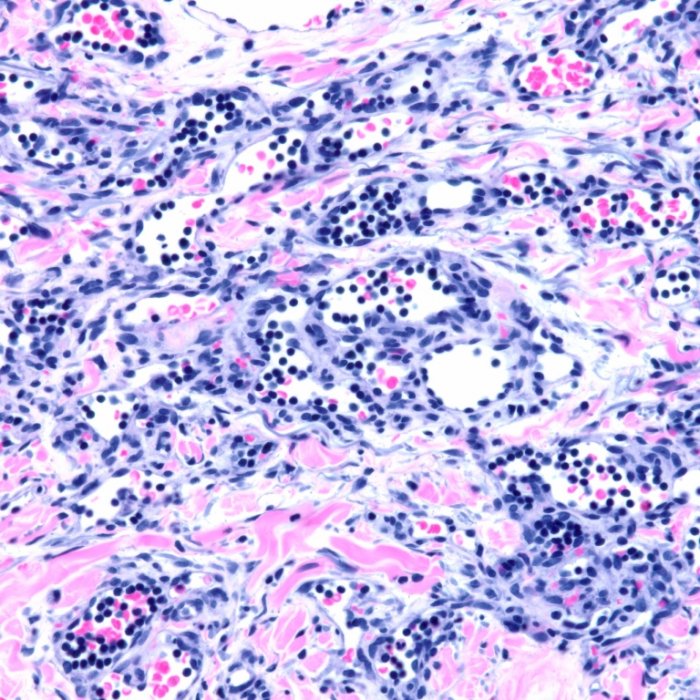
Advanced Dermatology Associates, LTD. (AD11-13464, 12/15/2011) Right medial and lateral breast: “Both specimens contain a proliferation of irregular, erythrocyte-containing, vascular channels that are lined by a single layer of flattened endothelial cells. These vary in size and shape with small jagged channels subtly intercalated between collagen bundles admixed with large ectatic ones. This process is most prominent in the superficial half of the dermis though it is full thickness, overall, with the involvement of the subcutis (right breast medial). Endothelial morphology is monomorphic with no cytologic atypia and no mitoses. Superimposed on this, and also most prominent is a conspicuous population of lymphocytes that are clustered within, and around, the vessels.”
Additional Studies: D2-40 negative, FISH for MYC gene amplification negative
October 2010: There are a number of ectatic vessels with plump small endothelial cells surrounded by a patchy mixed cell infiltrate. The infiltrate is composed of lymphocytes, histioctyes, and a rare eosinophil. Extravasated erythrocytes are present.

December 2011: Monomorphic endothelial cells with no cytologic atypia and no mitoses. There is a conspicuous population of lymphocytes clustered within and around the vessels.
DIFFERENTIAL DIAGNOSIS:
1. Atypical vascular lesion
2. Angiosarcoma
3. Radiation dermatitis


