
Presenter: Alyson Ridpath, DO
Dermatology Program: OhioHealth O’Bleness
Program Director: Dawn Sammons, DO, FAOCD
Submitted on: February 21, 2018
CHIEF COMPLAINT: New-0nset severe, pruritic, bullous eruption
CLINICAL HISTORY: A 67-year-old male with stage IV BRAF- and c-Kit-negative, NRAS-positive melanoma of unknown primary with metastases to the liver, lung and brain was started on nivolumab 3 mg/kg every two weeks. After 16 cycles over 32 weeks, he presented to the emergency department with a new, severe, pruritic, bullous eruption covering approximately 90% body surface area, and altered mental status. He was started on 1 mg/kg prednisone daily and betamethasone diproprionate 0.05% cream twice daily with the intention of restarting nivolumab after the steroid taper. His course was complicated by bacteremia and an inability maintain his BP on low dose corticosteroids. The inability to taper the patient to low dose steroids to disinhibit cellular immunity was a therapeutic challenge.
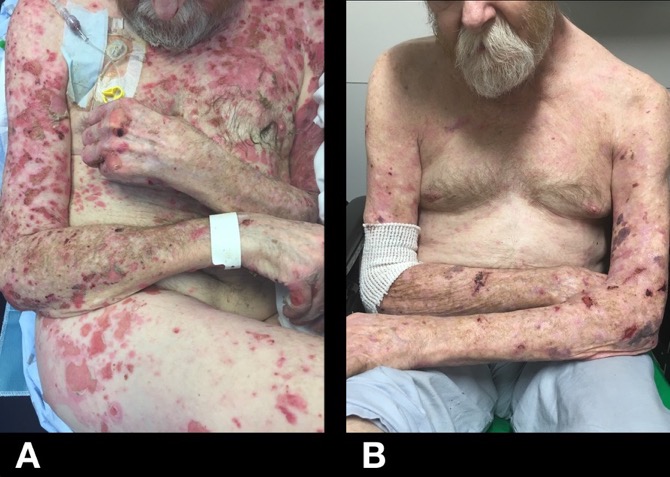
PHYSICAL EXAM:
Coalescent bullous eruption covering approximately 75% of body surface.
LABORATORY TESTS:
Labs were significant for autoantibodies to BP-180 > 150.00 units [<9<9
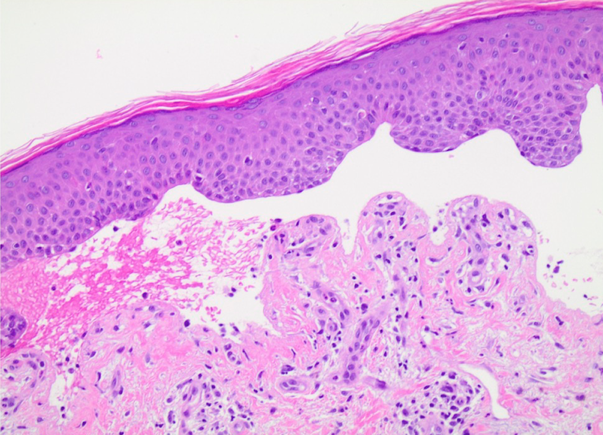
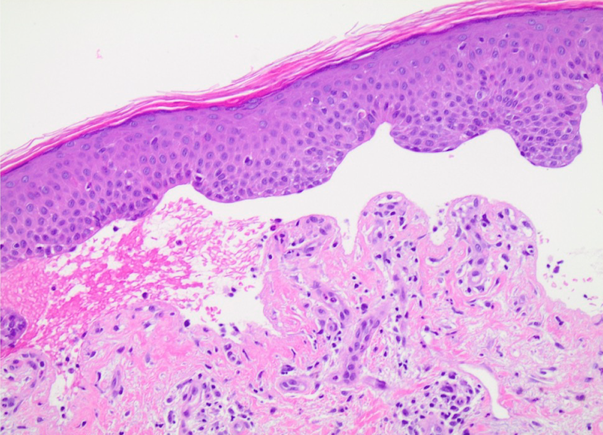
DERMATOHISTOPATHOLOGY:
Biopsy and direct immunofluorescence revealed a subepidermal bullous dermatosis with1+ linear IgG, C3 and C5b-9 deposition at the dermoepidermal junction, confirming a diagnosis of bullous pemphigoid.
DIFFERENTIAL DIAGNOSIS:
1. Age related bullous pemphigoid
2. Drug induced bullous pemphigoid
3. Lichen planus pigmentosus
4. Paraneoplastic pemphigus
5. Nivolumabu induced bullous pemphigoid


