

Presenter: Megan Goff, DO
Dermatology Program: WUHS/COMP AZ Derm program
Program Director: Stephen Kessler, D.O.
Submitted on: February 29, 2004
CHIEF COMPLAINT: Intermittent upper body eruption for several months
CLINICAL HISTORY: Patient presented to clinic with concerns of an intermittent, mildly pruritic upper body rash for several months. The patient believed it first appeared after a radiographic study with contrast for follow up of her metastatic breast carcinoma. The patient’s medical and surgical history was significant for left breast ductal carcinoma T1N0 status post modified radical mastectomy (8/86), metastasis to the mediastinum and retrocrural lymph nodes status post-chemotherapy completed 3/92, resection of left adrenal metastasis (10/92), and solitary brain metastasis, status post craniotomy, resection, X-ray therapy (10/96).
PHYSICAL EXAM:
The lesions consisted of multiple annular and polycyclic erythematous plaques with trailing scales over the face, neck, chest, abdomen, arms, and back. The lesions did not extend below the waistline.
The physical exam also revealed a slight cushingoid appearance. No lymphadenopathy of the neck or axillae was noted. Lungs were clear and the heart rate was regular. There was no lower extremity edema. Some mild tinea pedis was observed on both feet. The neurologic exam was normal.


LABORATORY TESTS:
A CT scan of the chest in August 1996 revealed a solitary 0.5 cm right lower lobe nodule. A repeat CT in April 1998 showed the nodule had increased to 1.5 cm. A third CT in July 1998 revealed the nodule to be stable at 1.5 cm.
DERMATOHISTOPATHOLOGY:
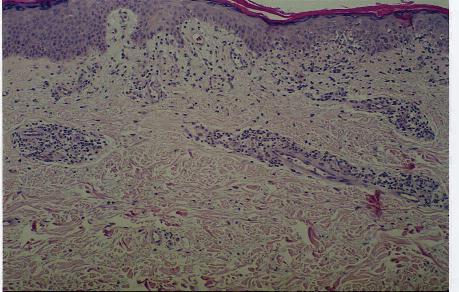
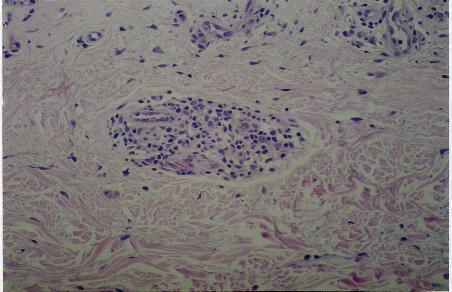
Microscopic description: A biopsy from the right shoulder demonstrated parakeratosis, spongiosis of the epidermis, and a cuffing superficial perivascular infiltrate of lymphocytes and histiocytes. Both periodic acid-Schiff (PAS) stains of the histology and potassium hydroxide (KOH) of the scale failed to reveal fungal elements.
DIFFERENTIAL DIAGNOSIS:
1. Granuloma annulare
2. Tinea corporis
3. Erythema annulare centrifugum
4. Lymphoma cutis


