

Presenter: Michelle Foley, DO, Brett Bender, DO, Joe Schneider, DO, John Coppola, DO, Brad Neuenschwander, DO, Derrick Adams, DO
Dermatology Program: Michigan State University POH Medical Center / Botsford Hospital
Program Director: Michael Mahon, DO
Submitted on: June 25, 2008
CHIEF COMPLAINT: “Painful sores on both hands”
CLINICAL HISTORY: A 41 yo Caucasian male presented to our clinic with the above chief complaint stating the lesions began to develop after he sustained an abrasion to his right third finger while at work. He began to note multiple similar lesions developing shortly thereafter and was admitted to a local hospital for presumed cellulitis. Unable to tolerate IV vancomycin, he was started on a short course of oral antibiotics and was referred to our service by the infectious disease physician for an evaluation to rule out presumed pyoderma gangrenosum. Hospital treatment consisted of IV vancomycin and an oral course of Bactrim without improvement. A two-week course of topical fluocinonide 0.1% cream and cephalexin 500mg TID was also unsuccessful. No pertinent past medical history. Social history included a 1-2 pk/day tobacco use, occasional ETOH with a history of remote abuse, no illicit drug use, and no recent travel. Family hx was unremarkable. Review of systems significant for three years unintentional thirty-pound weight loss. Due to a lack of medical insurance, this had not been investigated previously.
PHYSICAL EXAM:
Multiple, well-circumscribed, erythematous/violaceous, ulcerated pustular plaques of the bilateral dorsal hands



LABORATORY TESTS:
CBC: RBC of 3.57 (low). Hg 13.3 (low), MCV 117.4 (high), MCH 37.3 (high), RDW 18.3 (high)
RBC morphology: 2+ macrocytosis, 1+ anisocytosis, Burr cells and hypersegmented neutrophils
CMP: WNL
Slightly elevated triglycerides, cholesterol, & LDL
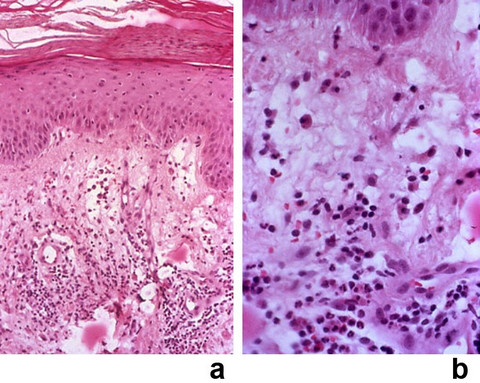
DERMATOHISTOPATHOLOGY:
4mm punch biopsy showed a neutrophilc infiltrate within the dermis. There was extensive papillary dermal edema. Blood vessels away from the neutrophilic infiltrate showed no evidence of acute vasculitis. There was some vascular damage in the areas of dense neutrophilia with leuckocytoclasis. PAS staining unremarkable.
DIFFERENTIAL DIAGNOSIS:
1. Bullous pyoderma gangrenosum
2. Deep fungal infection
3. Neutrophilic dermatosis of the dorsal hands
4. Erythema elevatum diutinum
5. Cutaneous small vessel vasculitis


