Presenter: Jason Mazzurco, DO; David Cleaver, DO; Brian Stewart, DO: Brooke Bair, DO; Billie Casse, DO
Dermatology Program: St. Joseph Mercy Hospital Ann Arbor/MSUCOM
Program Director: Dr. Daniel Stewart, DO
Submitted on: August 9, 2008
CHIEF COMPLAINT: “Itchy sores on hands and feet”
CLINICAL HISTORY:
Signs and symptoms: An 81-year-old white male with a significant past medical history of chronic renal failure, bladder cancer and hemochromatosis presented with a three to four-week history of “sores all over his body.” He complained of pruritus, scratching and picking at the lesions. He also complained of chronically decreased urine output and swelling in both feet.
Previous Treatment: He had previously been treated with diphenhydramine and hydroxyzine with little improvement of pruritus or skin lesions.
Other information: The rest of the review of systems was unremarkable. He has been on hemodialysis for approximately 5 years for which he has a fistula in his left arm for dialysis access and has no history of diabetes mellitus. His medications at presentation included tramadol, diclofenac, alprazolam, metoprolol, losartan, omeprazole, diphenhydramine, and hydroxyzine.
PHYSICAL EXAM:



Examination revealed multiple crusted and excoriated erosions and ulcers on the dorsal hands, arms, legs, and feet bilaterally. The erosions involved the patient’s left side more extensively, especially his left arm and dorsal hand. A few scattered excoriated papules with central keratotic plugs were also present. An arteriovenous fistula was noted in the left brachium.

LABORATORY TESTS:
CBC : WBC 4.5, HGB 12.5, HCT 36.5, Platelet 110
BUN 20, Creatinine 3.8, Albumin 2.6, ESR 22
Alk Phos, Calcium, Glucose, AST, ALT, Sodium, Potassium, ANA and were all WNL 24 hour urine porphyrins were not done due to patient’s inability to produce urine
DERMATOHISTOPATHOLOGY:
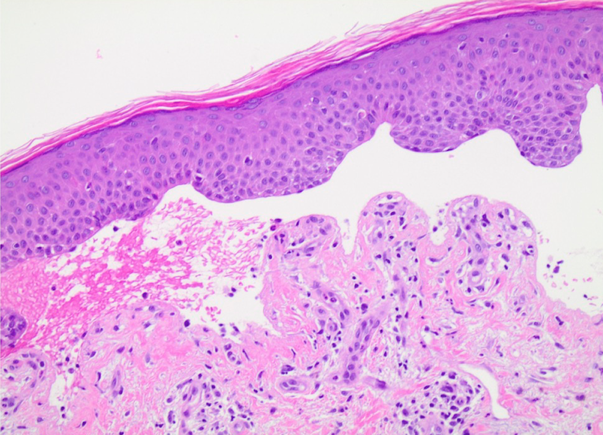
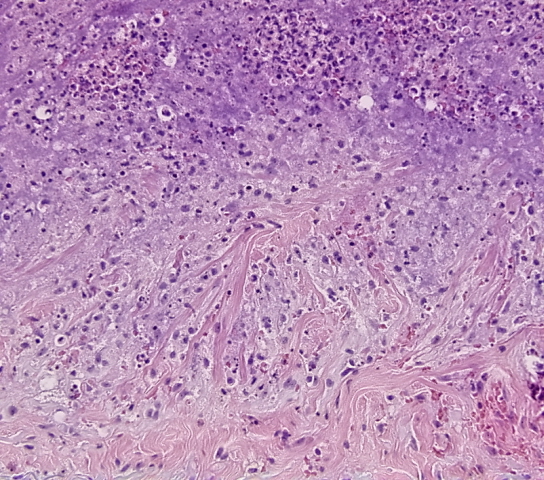
A punch biopsy of the right dorsal hand at the base of the fifth finger revealed a crater-like ulcer in the epidermis with scattered extravasation of collagen fibers through the ulceration. Neutrophils present at the base of the ulcer. A patchy perivascular lymphocytic infiltrate was seen within the dermis.


DIFFERENTIAL DIAGNOSIS:
1. Porphyria cutanea tarda
2. Acquired perforating dermatosis secondary to renal failure
3. Prurigo nodularis
4. Kyrle’s disease
5. Excoriations secondary to prurigo simplex