

Presenter: Shana Rissmiller, DO, Sarah Ferrer, DO, Emily Matthews, DO, Jamie Groh, DO
Dermatology Program: West Palm Hospital/ Palm Beach Consortium for Graduate Medical Education
Program Director: Dr. Robin Shecter, DO
Submitted on: May 19, 2014
CHIEF COMPLAINT: An evolving ulcerative lesion on the left forearm
CLINICAL HISTORY: A 51-year-old Colombian male presented to the office with an approximately 3-week history of an evolving ulcerative lesion on the left forearm. He first noticed the lesion shortly after returning from a 2-month recreational stay in Colombia. He denied any known trauma or arthropod assault. The lesion reportedly began as a non-pruritic erythematous papule. Over the course of the subsequent weeks, the area enlarged, ulcerated, and became crusted. He denied fever, chills, or abdominal pain.
Previous Treatment: Topical terbinafine
Other information: His past medical history was only significant for hypothyroidism which was being managed with Synthroid.
PHYSICAL EXAM:
Physical examination demonstrated an approximately 2.5 x 1.5 cm pink, crusted plaque with central ulceration and a raised border on the dorsal left forearm. There was no fluctuance, drainage, or sporotrichoid spread appreciated.

Left forearm 6 weeks into treatment:

LABORATORY TESTS: N/A
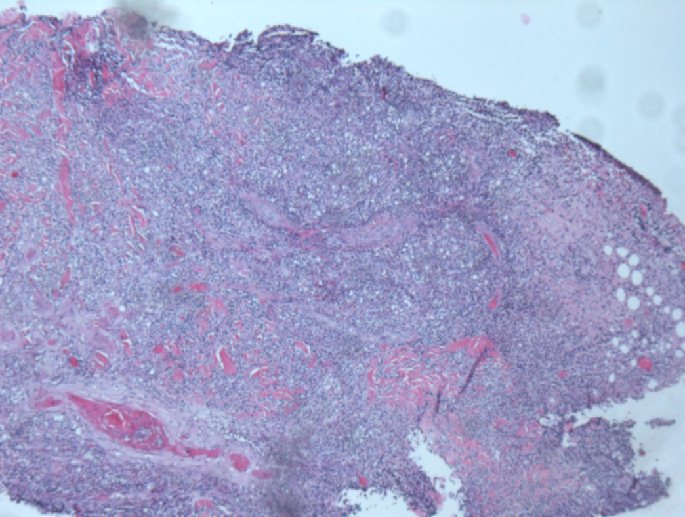
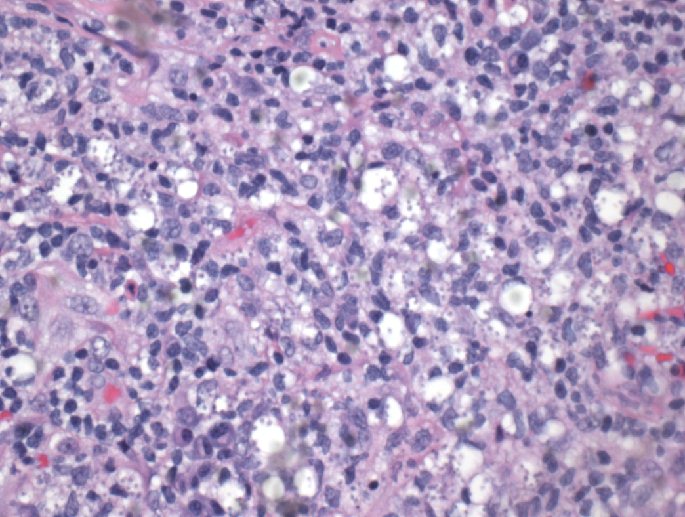
DERMATOHISTOPATHOLOGY:
A 3mm punch biopsy was performed. Histopathological evaluation demonstrated an ulcerated lesion with a mixed inflammatory infiltrate. Giemsa staining was also performed. At higher power, amastigotes were identified within dermal macrophages.
DIFFERENTIAL DIAGNOSIS:
1. Leishmaniasis
2. Ecthyma
3. Fungal
4. Atypical mycobacteria
5. Persistent arthropod reaction


