Presenter: Paul M. Graham
Dermatology Program: St. Joseph Mercy Dermatology
Program Director: Daniel Stewart, DO FAOCD
Submitted on: August 19, 2015
CHIEF COMPLAINT: Exquisitely painful nodules and marked edema of his bilateral lower legs
CLINICAL HISTORY: A 69-year-old Caucasian man presented with exquisitely painful nodules and marked edema of his bilateral lower legs. The nodules first appeared nine months ago and have shown a waxing and waning course. His past medical history includes chronic pancreatitis of unknown origin, hypertension, gastroesophageal reflux disease, inflammatory arthritis, and hypercholesterolemia. The patient reported experiencing painful skin nodules on his lower extremities for the past eight months, alongside joint pain and swelling in the metacarpophalangeal (MCP), metatarsophalangeal (MTP), and ankle joints. He had previously been treated with intralesional corticosteroid injections, which yielded only a marginal response. Additionally, he used high-potency topical corticosteroids and nonsteroidal anti-inflammatory drugs for symptomatic pain relief. Notably, the patient has a history of numerous hospital admissions for pancreatitis and is currently being managed by Rheumatology for his arthritic symptoms.
PHYSICAL EXAM:
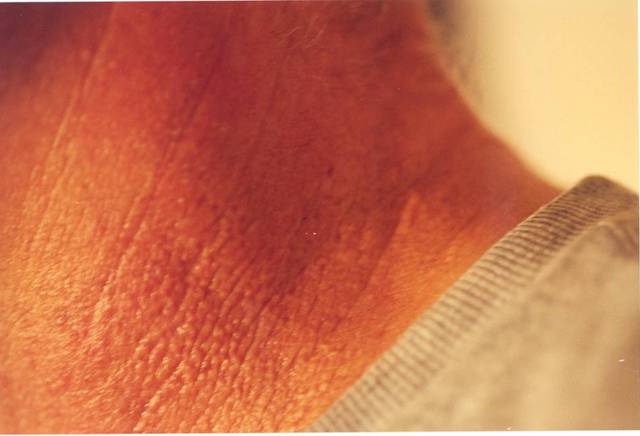
Physical examination revealed multiple 1-3 cm ill-defined, red to brown subcutaneous nodules on the bilateral lower legs and the right inferomedial thigh. There was no overlying ulceration, drainage, or bleeding. Marked erythema and edema of the right second, third, fourth, and fifth metacarpophalangeal (MCP) joints, left first metatarsophalangeal (MTP) joint, and bilateral ankles were observed. Diffuse 2+ pitting edema was present in the bilateral lower extremities.


LABORATORY TESTS:
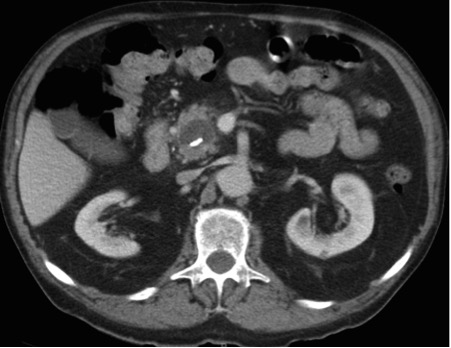
Laboratory results revealed increased amylase (5,250 U/L), lipase (9,197 U/L), ESR (94 mm/h), and CRP (93.5 mg/L). Triglycerides, AST, ALT, ANA, and RF were within normal limits. CT scan of the left ankle revealed cortical bony erosion of the calcaneus. CT scan of the abdomen and pelvis revealed a 1.8 x 1.4 cm hypodense lesion within the pancreatic head with calcifications and mild proximal pancreatic ductal dilation. Ultrasonography showed no evidence of cholelithiasis. Bone biopsy specimens demonstrated mild chronic inflammation with no evidence of osteomyelitis. A serum uric acid level was found to be 4.4 mg/dL and a joint aspirate demonstrated turbid fluid with lipoid material and no evidence of crystals or organisms on culture.
DERMATOHISTOPATHOLOGY:
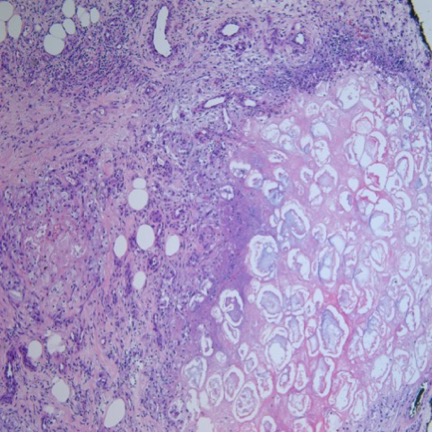
A 4mm punch biopsy of a nodule on the right leg revealed extensive lobular and septal liquefactive adipocyte necrosis with scattered neutrophils and lymphocytes. Aggregates of fine granular basophilic material were observed with prominent adipocyte degeneration and calcification.
DIFFERENTIAL DIAGNOSIS:
1. Alpha 1-antitrypsin deficiency panniculitis
2. Erythema nodosum
3. Nodular vasculitis
4. Polyarteritis nodosa
5. Lupus panniculitis