

Presenter: Leslie Marshall, D.O.
Dermatology Program: Northeast Regional Medical Center
Program Director: David Cleaver, D.O.
Submitted on: January 5, 2017
CHIEF COMPLAINT: “itchy rash”
CLINICAL HISTORY: A previously healthy, non-pregnant 22-year-old Hispanic female presented with a 5-day history of a pruritic eruption on her dorsal right hand, upper arms, and back. She had returned to the United States 4 days prior after a 2-week trip to Santa Anna, El Salvador. Her symptoms began one week after her arrival to El Salvador with neck swelling and general malaise. One day before returning home (day 7 of illness), she developed tenderness and swelling surrounding a mosquito bite on her right ankle followed by a rash on her arms, back, and thighs. Accompanying symptoms included arthralgias in her hands, a low-grade fever, headache, and paresthesias. She was prescribed a prednisone taper from the ER physician, which was not helpful. She reported being bitten several times by mosquitos while in El Salvador.
PHYSICAL EXAM:
Physical examination revealed tender right anterior cervical lymphadenopathy. Punctate erythematous follicular-based papules were scattered on the arms, back, and thighs. An erythematous papule with surrounding induration was present on the lateral right ankle. In addition, there was an annular, erythematous plaque with a fine scale on the dorsal right hand.



LABORATORY TESTS:
Positive Zika IgM Antibody ELISA performed by The Centers for Disease Control and Prevention (CDC) indicated ZIKV infection and was confirmed by neutralizing antibody testing. The initial real-time reverse transcription-polymerase chain reaction (rRT-PCR) was negative.
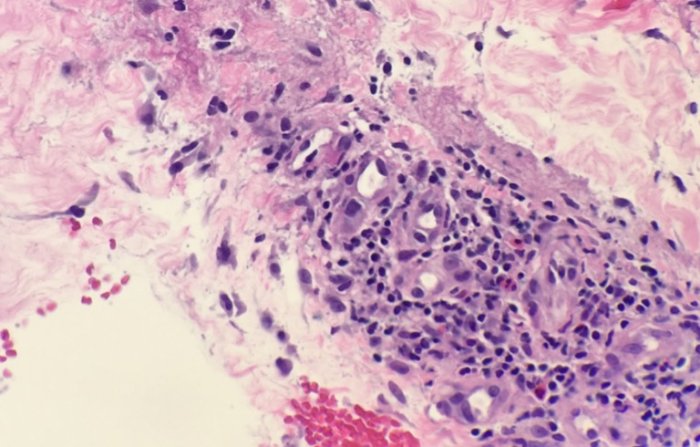
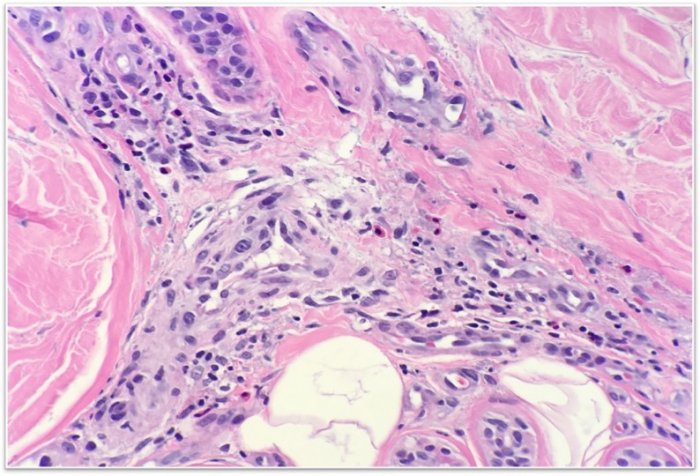
DERMATOHISTOPATHOLOGY:
Punch biopsy for histological analysis from the lateral ankle revealed superficial and deep perivascular lymphocytic infiltrate with dense infiltrate of eosinophils extending down to the dermal subcutaneous fat junction consistent with arthropod assault.
DIFFERENTIAL DIAGNOSIS:
1. Dengue Fever
2. Yellow Fever
3. Zika Virus
4. Chikungunya virus


