Presenter: Jonathan Bellew, DO
Dermatology Program: Advanced Desert Dermatology
Program Director: Vernon T. Mackey, DO
Submitted on: September 7, 2017
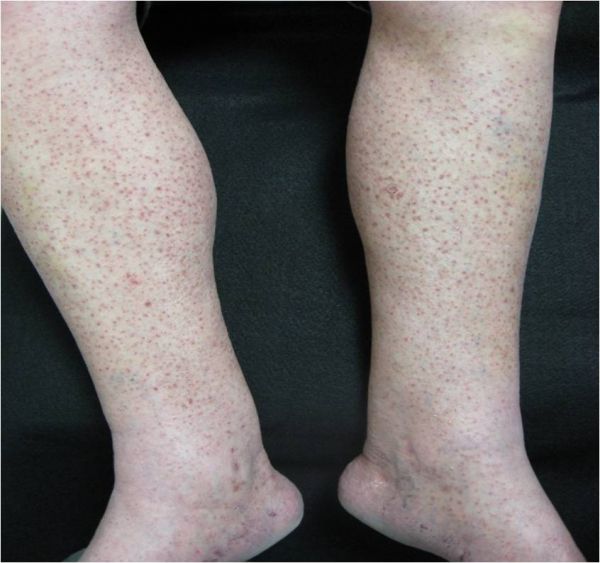
CHIEF COMPLAINT: Violaceous hyperpigmented rash on the right upper body
CLINICAL HISTORY: A 79-year-old Caucasian male presented to the outpatient office setting with a six-month history of progressive asymptomatic violaceous-black pigmented papules, plaques, and nodules of the right shoulder, axilla, chest, upper abdomen, and lateral trunk. The patient denied systemic complaints, pain, pruritis, or discomfort. Two months prior to the skin eruption the patient underwent primary resection of a right mid-back malignant melanoma. The melanoma was histologically classified as superficial spreading and nodular type with a Breslow’s thickness of 1.4 mm and Clark’s level IV, with no ulceration, lymphovascular invasion, or satellitosis. Sentinel node biopsy showed extension to the right axillary lymph nodes prompting axillary lymphadenectomy.
Other information: Past medical history included multiple non-melanoma skin cancers treated with wide excision on the left upper back (2006) and Mohs micrographic surgery on the right upper occipital scalp (2010), and lymphoma treated with chemotherapy and radiation 3 years prior. His family history was significant for lung cancer in both parents, as well as brain and breast cancer in his brother and sister respectively.
PHYSICAL EXAM:
On presentation, the excision scar at the right mid-back had signs of hypertrophic scarring, but no evidence of pigmentation or recurrence of melanocytic features. Over 100, non-tender, smooth, firm, 3 mm dark purple-brown-black papules were localized to the right shoulder, axilla, chest, and upper abdomen. There was no evidence of secondary skin lesion morphology. No palpable adenopathy was appreciated.




LABORATORY TESTS:
Complete blood cell count with differential, comprehensive metabolic panel, and lactic dehydrogenase levels was unremarkable.
DERMATOHISTOPATHOLOGY:
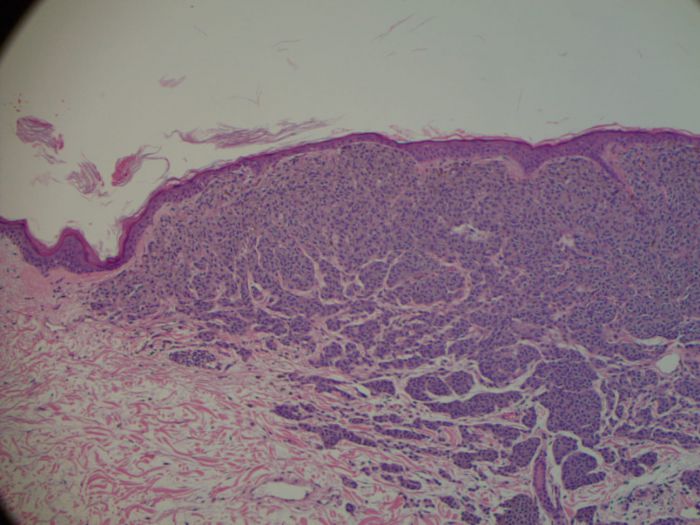
Histopathologic evaluation of two isolated lesions at the right chest wall via two 5 mm punch biopsies revealed extensive involvement of the papillary dermis demonstrating confluence of heavily pigmented pleomorphic melanocytic nests with an absence of maturation.
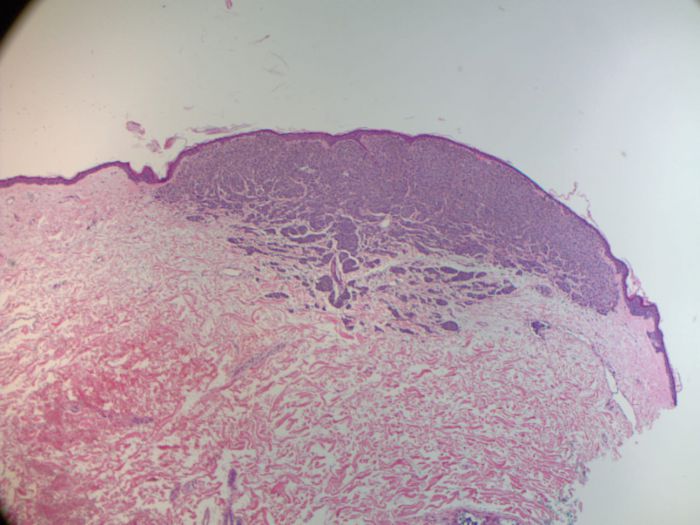
Additional microscopic features included; epidermal and adnexal sparing, thinning of the epidermis around melanocytes, flattening of rete ridges, prominent nucleoli with increased mitoses, and increased nuclear to cytoplasmic ratio.
Interestingly, a focal area of intravascular invasion was noted in the dermis representing angioinvasion.

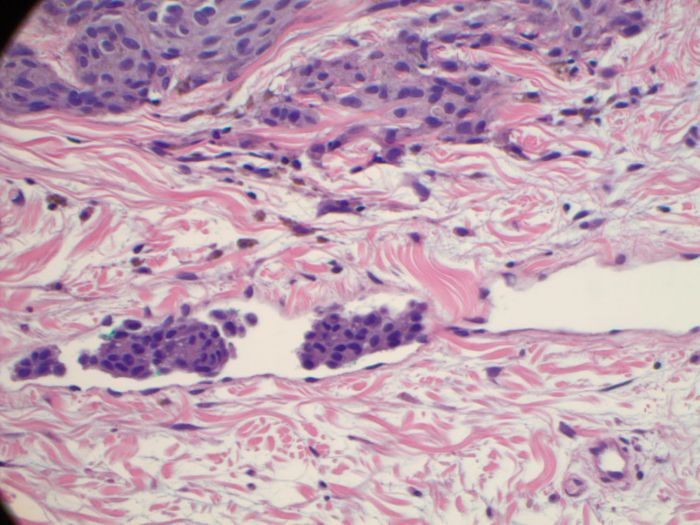
Immunostaining was positive for Pan Melanoma stain (HMB45/ MART-1/ tyrosinase). CD31 positivity was noted as well, confirming the intravascular focus of melanoma cells. Genetic testing failed to detect mutations in BRAF V600, EGFR, or NRAS.
DIFFERENTIAL DIAGNOSIS:
1. Lymphangioma circumscriptum
2. Angiosarcoma
3. Kaposi’s sarcoma
4. Lymphomatoid papulosis
5. Secondary syphilis