

Presenter: Michelle Elway, DO
Dermatology Program: Colorado Dermatology Institute/Rocky Vista University
Program Director: Reagan Anderson, DO
Submitted on: December 4, 2017
CHIEF COMPLAINT: new, growing lesion on her left cheek
CLINICAL HISTORY: A 12-year-old female was referred to our office by her Pediatrician complaining of a new, growing lesion on her left cheek. The patient and her mom reported that the lesion appeared approximately one month prior as a small reddish spot, which has since grown significantly. The patient denied changes in color, bleeding, ulceration, pain, pruritis, or crusting of the lesion. She also denied any systemic systems. They had no other concerns at that time. No previous treatments. The patient had no past medical history to note. Family history was non-pertinent.
PHYSICAL EXAM:
On physical exam, she was a well-appearing, pleasant female. A 1.8 x 2 cm erythematous indurated plaque on the left malar cheek was present. No other abnormal skin findings were noted.


LABORATORY TESTS:
A CBC with differential, complete metabolic panel, UA, LDH, uric acid, PT/PTT/INR, and an immunoglobulin profile were all performed and were within normal limits.
DERMATOHISTOPATHOLOGY:
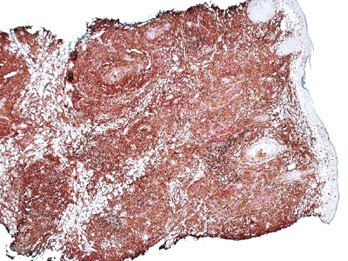
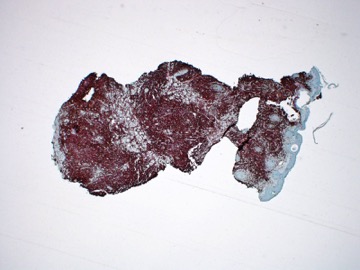
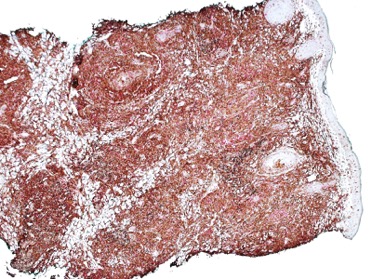
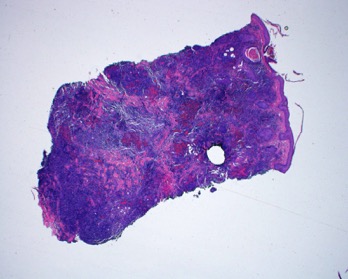
A 4mm punch biopsy was performed revealing a concerning process consisting of a dense mononuclear inflammatory infiltrate with a thin grenz zone. There were chiefly lymphocytes with a smaller number of acute and chronic inflammatory cells including some eosinophils and plasma cells. Given that the dense infiltrate was not specific for any one entity, further work-up was performed. Several special stains and immunohistochemical analysis were performed including CD1a demonstrating large number of antigen-presenting cells; CD3/CD20 (combo) showing relatively equal numbers of T-cells and B-cells, but importantly, the B-cells were not arranged in any type of germinal centers and were interspersed “randomly” throughout the process; CD4/CD8 (combo) demonstrated slightly more CD4 than CD8 positive T-cells; CD7 demonstrated positivity in the T-cells scattered throughout the process; CD30 showed no relevant positivity; CD56 demonstrated scattered positivity; EBER revealed no positivity. A B-Cell/T-Cell Clonality Screen was also performed revealing a T-Cell monoclonality with TCR gamma detected. However, a B-cell monoclonality IgK and IgH was not detected. Subsequently, the case was signed out as a large and “bottom-heavy” atypical lymphoid infiltrate, with documented T-cell clonality.
DIFFERENTIAL DIAGNOSIS:
1. Primary Cutaneous Small/Medium Pleomorphic CD4+ T-cell Lymphoproliferative Disorder, formerly Primary Cutaneous Small/Medium Pleomorphic CD4+ T-Cell Lymphoma
2. Pseudolymphoma/Atypical form of Lymphocytoma Cutis
3. Peripheral T-Cell Lymphoma, Unspecified
4. Angioimmunoblastic T-Cell Lymphoma
5. Tumor-stage Mycosis Fungoides


