Presenter: Jessica Kim DO
Dermatology Program: Palm Beach Consortium Graduate Medical Education
Program Director: Robin Shecter DO
Submitted on: April 27, 2018
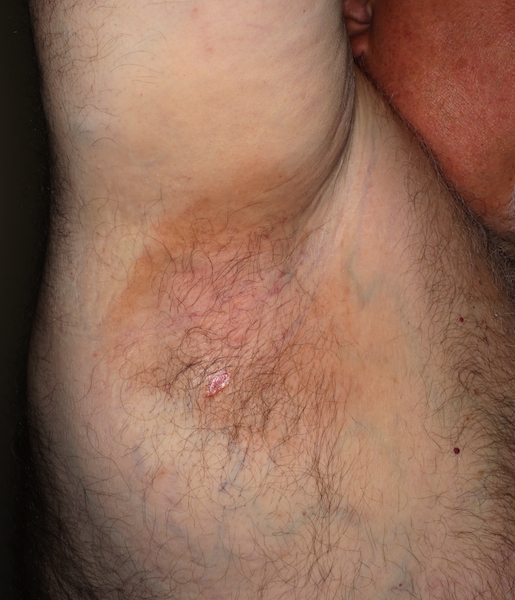
CHIEF COMPLAINT: Chronic bilateral axillary rash which developed over the course of a year
CLINICAL HISTORY: Patient presented with an asymptomatic rash localized to the axillae. Patient has tried changing deodorants and using talcum powder without improvement. Past medical history includes diabetes mellitus (HgA1c 6.2), hypothyroidism, stasis dermatitis, hand eczema and hypertension. Pt denies use of tobacco or illicit drugs. He is currently on levothyroxine, carvedilol, pregabalin, saxagliptin, tamsulosin, pantoprazole, glipizide, warfarin, lisinopril, metformin, and furosemide. His allergies include acetaminophen, morphine, hydromorphine, zocor, and niaspan.
PHYSICAL EXAM:
Vitals: BMI: 54.01 kg/m2, T: 98.7° F, P: 74 bpm, RR: 18, BP: 139/68
General: awake, alert, oriented, no acute distress
Fitzpatrick I. Bilateral axillae with erythematous papules coalescing into plaques. No weeping or blisters noted.



LABORATORY TESTS:
No additional lab tests were done. Most recent HgA1c was 6.2.
DERMATOHISTOPATHOLOGY:
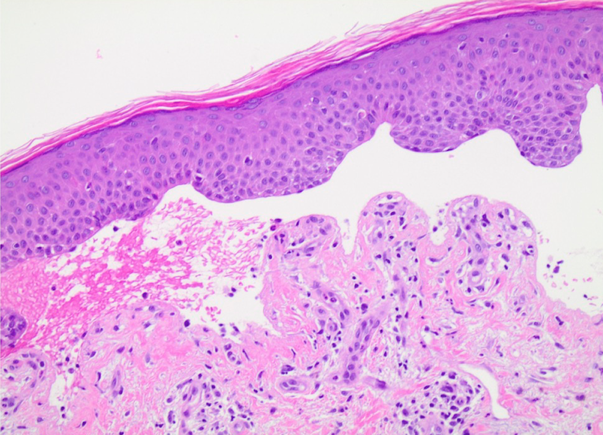
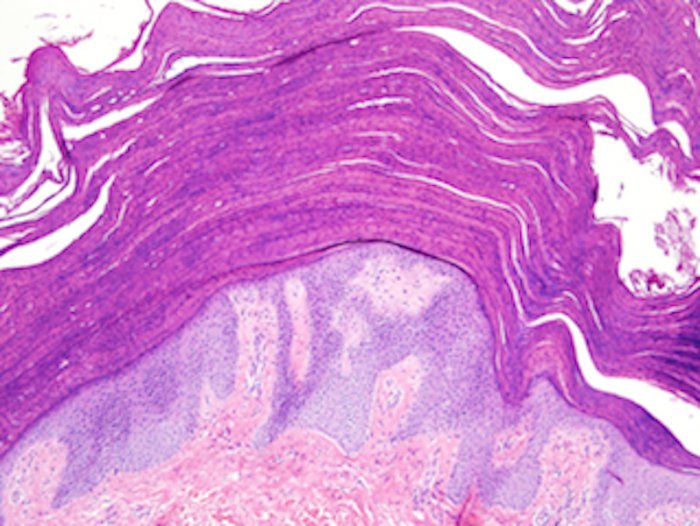
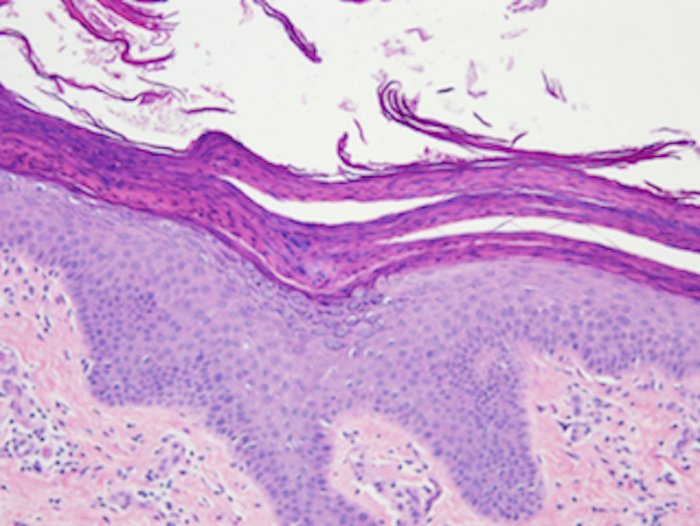
Shave biopsy of the right axilla showed thick parakeratosis with retention of keratohyalin granules and psoriasiform epidermal hyperplasia consistent with axillary granular parakeratosis.
DIFFERENTIAL DIAGNOSIS:
1. Allergic/ Irritant Contact Dermatitis
2. Intertrigo
3. Darier’s Disease
4. Hailey Hailey Disease
5. Acanthosis Nigricans