

Presenter: Christine Ku, DO; Michael Hohnadel DO; Rick Lin DO; Michael Sedrak MD.
Dermatology Program: South Texas Dermatology Residency Program, Bay Area Corpus Christi Medical Center
Program Director: Rick Lin, DO MPH
Submitted on: August 8, 2019
CHIEF COMPLAINT: ¨I have a rash and other lesions on my fingers”
CLINICAL HISTORY: The patient is a 23-year-old female who presented to the clinic with a complaint of diffuse skin rash and ulcerations. She reported symptom onset about 12 months ago, with worsening of symptoms in the past 4-6 months. Symptoms began with cuticle inflammation consisting of redness and pain. She saw her primary care physician who prescribed topical therapy with some improvement. A few weeks later she noted wrist pain and swelling followed by the progressive development of diffuse arthralgia and arthritis in fingers, hands, and knees. The patient then described onset of a rash over thighs and buttocks which then spread to her torso and extremities. She described the rash as pruritic and slightly painful. This was followed by the development of skin ulcerations resulting in open, non-healing wounds on extremities as well as digital ulcers on hands and oral ulcers. Of note, the patient also reported an unintentional weight loss of 20 pounds over the past year (over 15% of her initial body weight). The patient denied fevers, change in vision, shortness of breath or chest pain, or other systemic symptoms. The patient was evaluated by rheumatology who trialed prednisone, methotrexate injections, and Plaquenil with some improvement in symptoms. The patient had no other significant medical or surgical history, was previously not taking any medications. It was noted that she had a positive family history of lupus in her maternal aunt and cousin.
PHYSICAL EXAM:
On physical exam, the patient is a slender female who notably appears cachectic. She presents with an erythematous rash on the face in a malar distribution. There are diffuse macules, papules, and plaques across proximal and distal extremities and torso. The most striking cutaneous findings appear to be full thickness ulcers with a 2x3cm ulcer located on the posterior left shoulder, and smaller ulcers scattered over upper extremities including elbows. Hands demonstrated purplish discoloration of fingers without gangrene, left 2nd digit dactylitis, ulcers over left and right MCP joints and left 2nd PIP, and tortuous vessels around nail beds.




LABORATORY TESTS:
Initial lab work at time of visit was remarkable for a positive antimyeloperoxidase (MPO) antibody, significantly elevated AST and ALT (231 and 359 respectively), elevated LDH (342), ESR(39), and aldolase (25.6). Pertinent negatives included negative ANA, Scl-70, RNA Pol III, Jo1, SM-scl, SS-A/SS-B, dsDNA, ANCA, APL antibodies. CBC and CMP were largely unremarkable with exception of mild thrombocytopenia.
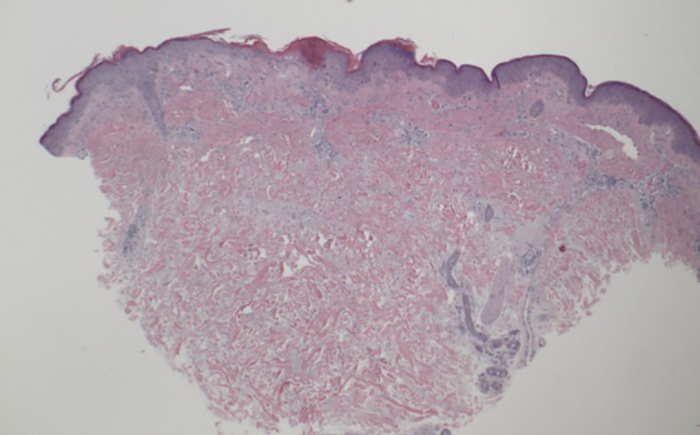
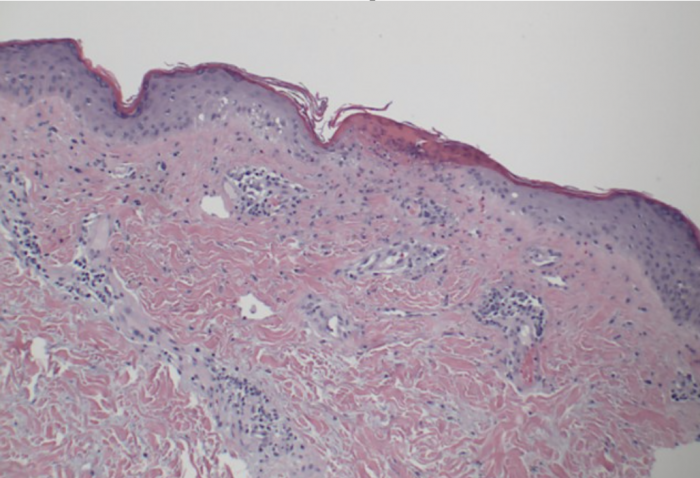
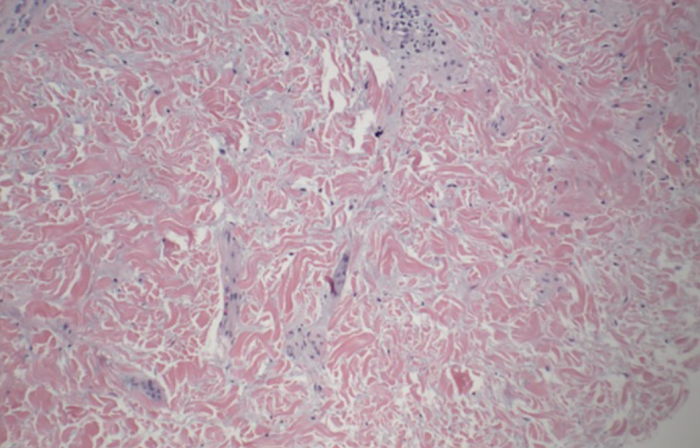
DERMATOHISTOPATHOLOGY:
We performed a skin biopsy of a lesion on the patient’s right thigh. Histopathology showed interface dermatitis with increased dermal mucin. Two immunofluorescence biopsies were both negative. A previous skin biopsy performed with another dermatologist demonstrated leukocytoclastic vasculitis showing inflammatory cell infiltrate, and nuclear dust with minimal fibrin in the wall of small blood vessels.
DIFFERENTIAL DIAGNOSIS:
1. Mixed connective tissue disease
2. Systemic sclerosis + Dermatomyositis
3. Diffuse scleroderma
4. Systemic Lupus Erythematosus
5. Polymyositis


