
Presenter: Valeria González-Molina, MD, Thomas L Davis, MD, Rick Lin, DO
Dermatology Program: South Texas Dermatology Residency, HCA Healthcare Corpus Christi Medical Center – Bay Area Program
Program Director: Rick Lin, DO MPH FAOCD
Submitted on: March 20, 2024
CHIEF COMPLAINT: “I have a rash all over my body and felt sick the past few days”
CLINICAL HISTORY: An 18-year-old Hispanic female presented to our clinic with diffusely spread, erythematous plaques and pustules covered by crusts, which had evolved over the past eight months. She denied any mucosal involvement but reported significant symptoms over the last three days, including difficulty walking, fever, skin tenderness, malaise, arthralgia, and headaches. Notably, no one else in her household exhibited similar lesions. The patient denied recent travel, sick contacts, alcohol use, illicit drug use, or smoking.
Of note, she had been admitted to the hospital one week prior to this visit due to concerns about a burn or drug reaction. During her hospitalization, she was started on high-dose oral steroids and was currently taking 10 mg of prednisone daily. Additionally, she had been applying over-the-counter Caladryl lotion to her entire body. The patient denied any known allergies to medications.
PHYSICAL EXAM:
Physical examination demonstrated erythematous, crusted, and confluent plaques and pustules diffusely spread across the body, sparing extensor and acral surfaces. No oral involvement.









LABORATORY TESTS:
The patient’s laboratory results indicated leukocytosis, mild anemia, elevated ESR and CRP, negative ANA and RF.
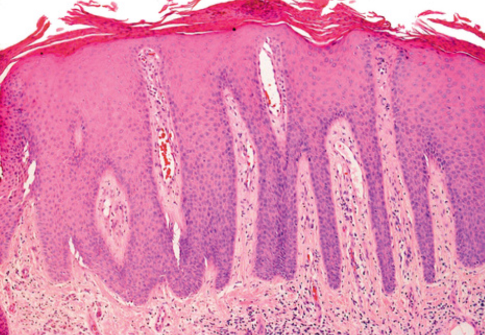
DERMATOHISTOPATHOLOGY:
Histopathological examination demonstrated confluent mounds of parakeratosis in the epidermis, characterized by pustular aggregates of neutrophils within and beneath the stratum corneum, known as Munro microabscesses. The findings included regular acanthosis with elongated rete ridges, thinning of the suprapapillary plates, and dilated capillaries in the papillary dermis, which are consistent with the inflammatory changes observed in generalized pustular psoriasis.
DIFFERENTIAL DIAGNOSIS:
1. Generalized Pustular Psoriasis
2. Acute Generalized Exanthematous Pustulosis (AGEP)
3. Subcorneal Pustular Dermatosis (Sneddon-Wilkinson Disease)
4. Steven-Johnson Syndrome/Toxic Epidermal Necrolysis
5. Pemphigus Foliaceus
6. Drug Reaction
7. Reactive Arthritis


