CORRECT DIAGNOSIS:
Epithelioid Angiosarcoma
DISCUSSION:
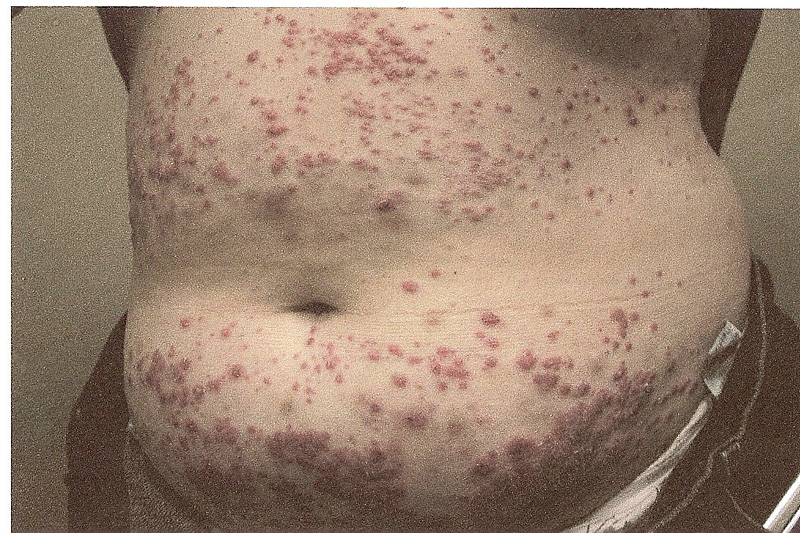
Angiosarcoma is a high-grade malignant neoplasm arising from endothelial cells, primarily affecting elderly Caucasian men aged 60 to 71. Approximately 50% of cases involve the head and neck region. Patients typically present with initially benign, bruise-like patches on the central face, forehead, or scalp, which may be accompanied by facial swelling or edema. As the disease progresses, lesions can develop into violaceous nodules that bleed easily and ulcerate, often spreading centrifugally and covering extensive areas of the head and neck, significantly impacting the patient’s quality of life.
The pathogenesis of angiosarcoma involves the clonal proliferation of malignant endothelial cells, with key angiogenetic genes implicated, including MYC gene amplification and mutations in protein tyrosine phosphatase receptor type B and phospholipase C gamma 1. This neoplasm has a poor prognosis, with only 30-60% of patients surviving beyond five years.
Angiosarcomas are most commonly observed on the breast in the context of post-radiation exposure. Stewart-Treves syndrome specifically describes angiosarcomas associated with lymphedema following mastectomy and lymph node dissection, frequently occurring on the inner aspect of the arm.
Diagnosis is confirmed through skin biopsy, revealing histological features characteristic of epithelioid angiosarcoma, including poorly circumscribed and highly infiltrative dermal tumors. The angiomatous areas display an irregular network of vessels dissecting through the dermis, lined by crowded, atypical endothelial cells, which may also contain intraluminal papillary projections. Solid areas may consist of poorly differentiated sheets of spindle- to polygonal-shaped cells, which can be difficult to differentiate from other malignancies, such as melanoma. Notably, C-myc amplification is found in radiation-induced angiosarcomas but is absent in atypical vascular lesions.
TREATMENT:
Treatment for angiosarcoma typically involved wide local excision of the tumor whenever feasible, aiming to achieve clear margins to reduce the risk of recurrence. If the surgical margins were compromised, adjuvant radiation therapy was recommended to target any remaining malignant cells. In cases where the angiosarcoma was unresectable or had metastasized, systemic chemotherapy was indicated, with paclitaxel often being the chemotherapy agent of choice due to its efficacy against vascular tumors. Our patient was referred to Texas Oncology for specialized management, where a multidisciplinary team—including surgical oncologists, medical oncologists, and radiation oncologists—collaborated to optimize her treatment plan. Regular follow-up was deemed crucial to monitor for recurrence or metastasis and ensure the best possible outcomes.
CONCLUSION:
Angiosarcoma, though rare, poses significant diagnostic and therapeutic challenges. Awareness of its clinical features and histological characteristics is crucial for timely diagnosis and intervention. The seemingly harmless clinical appearance of these tumors often contributes to delays in diagnosis and treatment. As the tumor grows, patients may experience more severe symptoms, including ulceration, bleeding, tissue infiltration, swelling, and tumor fungation. Additionally, the tumor’s invasion into nearby structures can complicate surgical procedures, resulting in unclear resection margins and significant soft tissue defects after radical resection, which pose further challenges for recovery and reconstruction.
Our case underscores the importance of early recognition and prompt referral, as demonstrated by the patient’s referral to Texas Oncology. The treatment approach typically involves wide local excision, adjuvant radiation therapy when necessary, and systemic chemotherapy for unresectable or metastatic disease. A multidisciplinary team is essential to provide comprehensive management and optimize outcomes. Given its aggressive nature and poor prognosis, early recognition and appropriate management are vital to improving outcomes for affected patients, along with ongoing follow-up to monitor for recurrence and manage complications effectively.
REFERENCES:
Spiker AM., Mangla A., Ramsey ML. Angiosarcoma. StatPearls [Internet]. Treasure Island (FL). StatPearls Publishing. 2024 Jul.
Cao, J., Wang, J., He, C., & Fang, M. Angiosarcoma: a review of diagnosis and current treatment. American journal of cancer research. 2019 Nov; 9(11), 2303–2313. [PMID 31815036]
Kim, WJ., & Kim, HK. Current understanding of angiosarcoma: disease biology and evolving treatment. Archives of craniofacial surgery. 2023 Oct; 24(5):203–210. [PMID 37919906]
Cui, L., Zhang, J., Zhang, X., Chang, H., Qu, C., Zhang, J., & Zhong, D. Angiosarcoma (Stewart-Treves syndrome) in postmastectomy patients: report of 10 cases and review of literature. International journal of clinical and experimental pathology. 2015 Sep; 8(9):11108–11115. [PMID 26617830]
Kumar, R., & Tiwari, S. (2020). Angiosarcoma: Clinical features, diagnosis, and management. Clinical Oncology, 32(12), 789-797. https://doi.org/10.1016/j.clon.2020.09.006. [PMID: 32927061]
Rosen, T., & Delman, H. (2021). Angiosarcoma: Clinical features and management. Journal of the American Academy of Dermatology, 84(5), 1369-1374. https://doi.org/10.1016/j.jaad.2020.10.021. [PMID: 33184925]
Becker, W. (2019). Angiosarcoma in the context of lymphedema: A clinical review. The American Journal of Surgery, 217(4), 667-672. https://doi.org/10.1016/j.amjsurg.2018.09.020. [PMID: 30359495]
Hoffman, A., & Kelsey, R. (2020). Post-radiation angiosarcoma: A clinical overview. BMC Cancer, 20(1), 365. https://doi.org/10.1186/s12885-020-06909-6. [PMID: 32389680]