
Presenter: Donna Tran, DO
Dermatology Program: Western University / College Medical Center
Program Director: Navid Nami, DO, FAOCD
Submitted on: January 5, 2014
CHIEF COMPLAINT: hardening of back
CLINICAL HISTORY: A 65-year-old gentleman presented to our dermatology clinic with complaints of hardening of his back. Painless, progressive hardening of his upper back present for years. He denied any associated symptoms. Denied any previous treatment. Past medical history was significant for insulin-dependent diabetes mellitus.
PHYSICAL EXAM:
Physical examination revealed a symmetrical, erythematous, indurated plaque with indistinct borders involving his posterior neck and upper back. No restriction in range of motion of the shoulders and neck was noted.

LABORATORY TESTS: N/A
DERMATOHISTOPATHOLOGY:
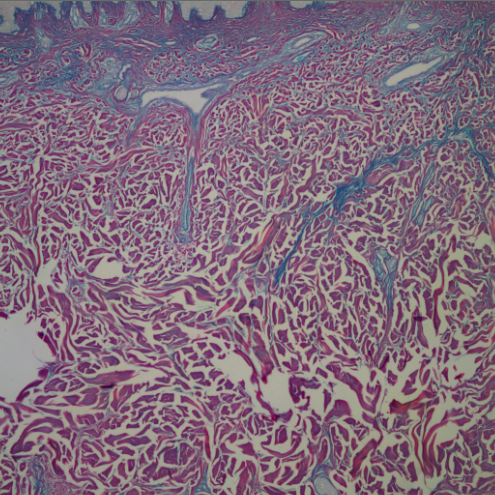
Histopathologic examination of a punch biopsy specimen revealed an intact epidermis with no interface changes. A scant superficial perivascular lymphocytic infiltrate was present.
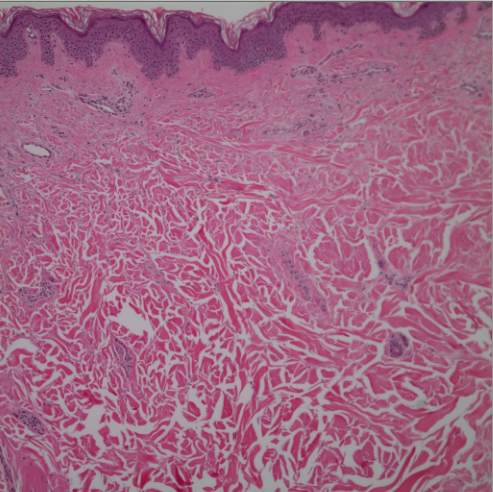
A colloidal iron stain revealed an increase in dermal mucin.
DIFFERENTIAL DIAGNOSIS:
1. Morphea
2. Cellulitis
3. Scleredema
4. Scleromyxedema
5. Scleroderma


