Itchy Patches
Presenter: Tracy Favreau, DO; Asfa Akhtar, DO; Merrick Elias, DO; Kristen Aloupis, DO; David Bonney, DO; Brian Feinstein, DO; Chris Buckley, DO; Marcus Goodman, DO; Allison Schwedelson, DO
Dermatology Program: NSUCOM/NBHD
CHIEF COMPLAINT: intensely pruritic lesions
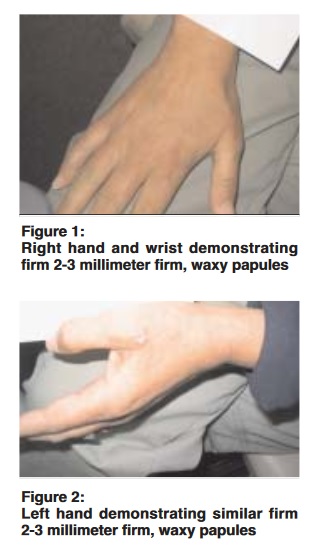
CLINICAL HISTORY: The patient is a 60-year-old Latin male presenting for evaluation of itchy patches in his bilateral axillae, inguinal region, and gluteal folds. The patient states this eruption is ongoing for the previous three months and is progressively worsening. Has not tried any topical or oral OTC or prescription medications to treat the lesions. He feels as if the lesions began after starting a new medication. He started taking Lipitor, Metformin, and Lotrel four months prior to the onset of lesions.